




"Thank you so much for being there for those who have no direction, nor support regarding a possible abortion."Donna - RTLCA Supporter
When the moment feels impossible, we're the people who stay.
Right to Life of Central California meets mothers, students, and families with practical help, compassionate presence, and a clear voice for the dignity of every human life.

We engage, equip, and embrace our community.
RTLCA is a local, life-affirming organization serving Fresno and the wider Central Valley through outreach, education, healing, and direct connections to care.
Our work is public and personal: we speak for the vulnerable, provide resources for families in crisis, train the next generation to understand human dignity, and walk with women and men carrying grief after abortion and pregnancy loss.
The path is simple: learn the mission, see the impact, find the right way to help, and take one meaningful next step.
16 Mothers chose life last year.
5,600 Parents and students reached annually.
35+ Women and men received healing annually through Rachel's Vineyard.
A connected response for real moments of need.
Each pathway helps people find the next right step: sidewalk presence, age-aware education, and confidential healing after abortion and pregnancy loss.
Three hundred neighbors. One sustaining commitment.
The 300 are the people who decided the work of Right to Life of Central California was worth their
generous, monthly support, about a dollar a day that keeps this work showing up all year long.
Be one of The 300.
Why Right to Life CA?
"A human's a human no matter how small. Thank you for teaching the importance of a baby and a baby matters!"Shared by a 3rd grade student after one of our presentations
"I believe in the mission here; I believe in caring about mothers who are in crisis and their babies. Letting them know they are not alone."Andria - Sidewalk Volunteer
Sidewalk Stories
The latest stories from the LIFEHOUSE sidewalk.
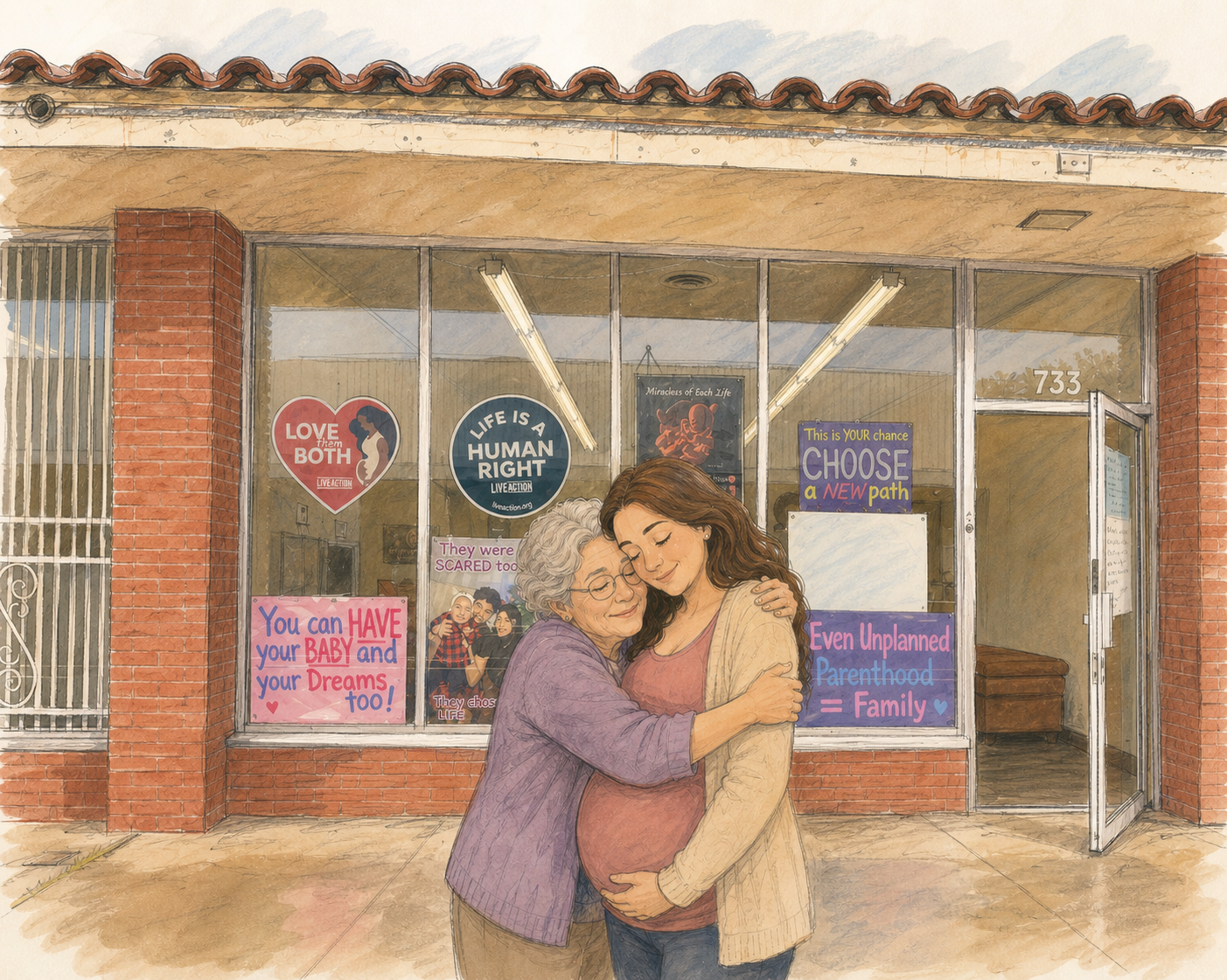
No One Walks This Alone
A young woman walked into an abortion clinic nineteen weeks pregnant. Her grandmother refused to let her face it alone, and a LIFEHOUSE team on the sidewalk helped the whole family walk out with a plan, a playpen, and a baby still on the way.
Read more
Sidewalk Story: Kiana
Kiana was five months pregnant when she connected with LIFEHOUSE. What began as one moment of help became months of steady support.
Read more
Sidewalk Story: Harmony
Harmony had already made up her mind to have an abortion. The team met her with honest conversation and no pressure, and in her own time she saw a future she had not dared imagine and chose life. Her baby girl is thriving.
Read moreThe newest impact numbers show what steady local support makes possible.
Read the reportRead our May Update
Read the update
We are building a culture where every life is protected and every family can find help.
RTLCA's work stays simple on purpose: engage the public, equip the community, and embrace the people directly in need.
Engage
Speak clearly in the public square, at events, on radio, and through local outreach.
Equip
Provide education resources and training so families and students can defend life with confidence.
Embrace
Connect women, men, and families to help, healing, prayer, and practical community support.
Stay Connected
Stay close to the work, and the lives being changed because of it.
Get email and text updates from Right to Life CA. Add your email, your mobile number, or both. Sharing your information is always optional and is never required to donate, register, or receive help.